
LNT (lymph node transfer) or free lymph node transplant is a supermicrosurgical technique aimed at clinical improvement in patients with advanced lymphoedema. The main point of the procedure is to harvest lymph nodes from an unoperated area and then transfer and implant them into the area of greatest lymphoedema. The new lymph nodes act as a suction-and-pressure pump – draining lymph from the lymph-damaged area. The effects are visible after 6-9 months.
Who is a patient for LNT?
Patients are eligible for free lymph node transplantation if we are unable to visualise active lymphatic pathways on previous imaging studies (lymphoscintigraphy, and lymphography using ICG) and clinically the lymphoedema is not reversible in response to conservative treatment. We often use this technique in patients in whom the effect of LVA is insufficient. There is the option of combining breast reconstruction with a DIEP flap and lymph node transfer. We operate on patients with secondary oedema after oncological, surgical and orthopaedic treatment, after trauma, as well as on patients with primary oedema of undetermined aetiology. We perform the ICG examination on our own in Słupsk, for the lymphoscintigraphy the patient is referred to the Nuclear Medicine Department of the Polish Red Cross Maritime Hospital in Gdynia.In order to be eligible for surgical treatment, the patient must independently apply conservative lymphoedema treatment techniques and be directed and supervised for by a physical therapist.
How to assess the status of lymphatic duct damage? Am I eligible for LNT?
To assess the lymphatic pathways, the patient undergoes a physical examination and ICG lymphography is performed – see ICG lymphography. The patient is also referred for lymphoscintigraphy. Based on the results obtained, s/he is eligible for surgical treatment. Once eligible, s/he must undergo computed tomography angiography (CTA) of the area to be operated. With the complete set of examination results, the patient comes to set the date of the surgery.
What does the LVA procedure technically consist in?
The patient is placed under general anaesthesia. On the basis of CTA and Doppler ultrasound performed intraoperatively, we identify an arterial and venous vessel in the area of oedema, to which we sew a nodal graft. Next, we harvest lymph nodes from a selected area and implant them in the area with oedema by making an arterial, venous and sometimes also lymphatic anastomosis. A drain is placed in the place where the lymph nodes are removed. Wounds are closed in layers.
From which area are the lymph nodes removed?
The lymph nodes are removed from a non-operated area, usually the inguinal region (superficial inguinal lymph nodes) or the axillary fossa. In exceptional cases the lymph nodes can be removed from under the chin, supraclavicular region or from a bigger network. The decision as to where to harvest the lymph nodes is made together with the patient preoperatively.
Can swelling occur in the area from which the lymph nodes are harvested?
The risk of lymphoedema in the area where the lymph nodes are harvested is minimal at 1-2%. To minimise the risk of damage to the lymphatic pathways that will translate into clinical lymphoedema we perform axillary reverse mapping (ARM) in every patient, (see ARM).
How long does this treatment last? Is it burdensome for me?
The procedure takes between 4-8 hours depending on anatomical conditions and the place where the lymph nodes are removed. To shorten it, we work on two microscopes simultaneously. The procedure is not burdensome, the whole procedure is carried out in superficial tissues. The patient suffers minimal pain and leaves for home on day 4 or 5.
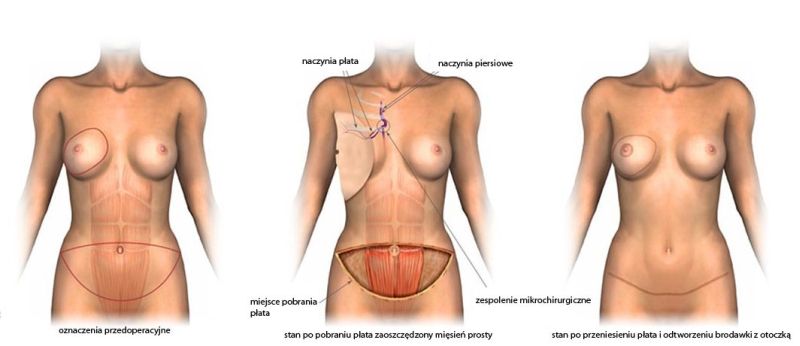
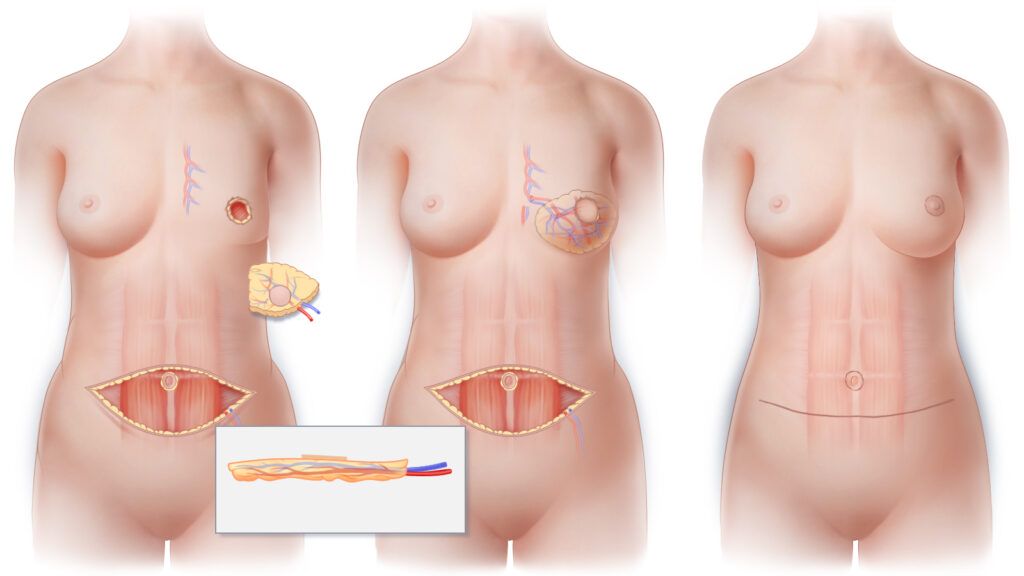
Can a DIEP flap be combined with lymph node transfer?
Of course, if you are eligible for the DIEP flap reconstruction and you have upper limb lymphedema on the operated side, come in for a consultation to discuss the option of combining the two procedures. In patients eligible, during the DIEP flap harvesting process, we also harvest the superficial inguinal lymph nodes and transfer them with the flap to the axillary fossa. Such a procedure enables comprehensive reconstruction of the breast elevation as well as simultaneous reconstruction of the lymphatic system.
Preparation for the procedure
- Dalacin C 300 mg three times daily – please start taking it 3 days before the surgery
- Before the surgery it is recommended to reduce the upper limb as much as possible (DLM). If the oedema is persistent, min. 3 days of Comprehensive Anti-Oedema Therapy
- Intensive work under supervision of a physical therapist on the limb in the 3rd and 2nd week before the surgery
- One week before surgery – compression therapy until surgery
- Please report to hospital with: blood group, blood tests: blood count, electrolytes, clotting times, creatine, chest X-ray
Post-operative care
Even before surgery, schedule (and possibly make) follow-up appointments 1,3,6,12 months after surgery!!!
Recommendations after LNT of the upper limb
- Get plenty of rest during the first week after surgery.
- Daily disinfection of the surgical wound
- The dressings must be changed daily for 1 week.
- Antibiotic for 7 days (Dalacin C 300 x 3/day)
- Physical therapy starting 3 weeks after the operation and after 3 weeks Manual Lymphatic Drainage is recommended bypassing the operated area.
- A grade 2 compression sleeve is recommended until approximately 6 months for a follow-up visit and potential ICG.
Recommendations after LNT of the lower limb
- Get plenty of rest during the first two weeks after surgery.
- Daily disinfection of the surgical wound
- The dressings must be changed daily for 1 week.
- Showering is allowed, yet the wound cannot ‘soak’ in water
- Antibiotic for 7 days (Dalacin C 300 x 3/day)
- Physical therapy starting 3 weeks after the operation. After 3 weeks Manual Lymphatic Drainage is recommended bypassing the operated area.
- A grade 3 compression stocking is recommended up to 6 months after surgery (of course it all depends on the type of lymphedema)
