
Our patients often ask whether we can reduce the risk of upper limb lymphoedema on the operated side in the group of patients in whom we have to remove the sentinel node or “all” lymph nodes of the axillary fossa. This risk is actually 13-77% with lymphadenectomy and 0-13% with sentinel lymph node removal. To reduce the risk of oedema in our patients we perform ARM.
Axillary reverse mapping (ARM) procedure claims to map and preserve arm lymphatic drainage during ALND and/or during SLNB, and then attempting to preserve them during the process of removing the lymph nodes. In a nutshell, we try to remove the lymph nodes responsible for the lymphatic drainage from the breast, at the same time taking special care not to unnecessarily damage the lymphatic pathways responsible for the lymphatic drainage from the “arm”. The concept of ARM has been known for a long time, but the introduction of indocyanine green (ICG) to map lymphatic pathways has significantly increased the effectiveness of the ARM procedure in reducing the risk of lymphoedema in breast cancer patients. In practice, the procedure involves administering indocyanine green intradermally to the anaesthetised patient at specific points of the ‘arm’ and then using appropriate equipment to visualise the lymphatic pathways (FIGS 1 and 2). When removing lymph nodes, we try to avoid “cutting” the lymphatic pathways glowing green.
A literature analysis conducted by Dutch researchers in 2016 considered 31 published scientific papers on ARM. The conclusions stated that axillary reverse mapping provides a technically simple, effective and oncologically safe way to reduce the risk of lymphedema.
At your consultation, ask if an ARM can be carried out on you?
Or maybe you are eligible to have your absorption pathways checked using indocyanine green (ICG)?

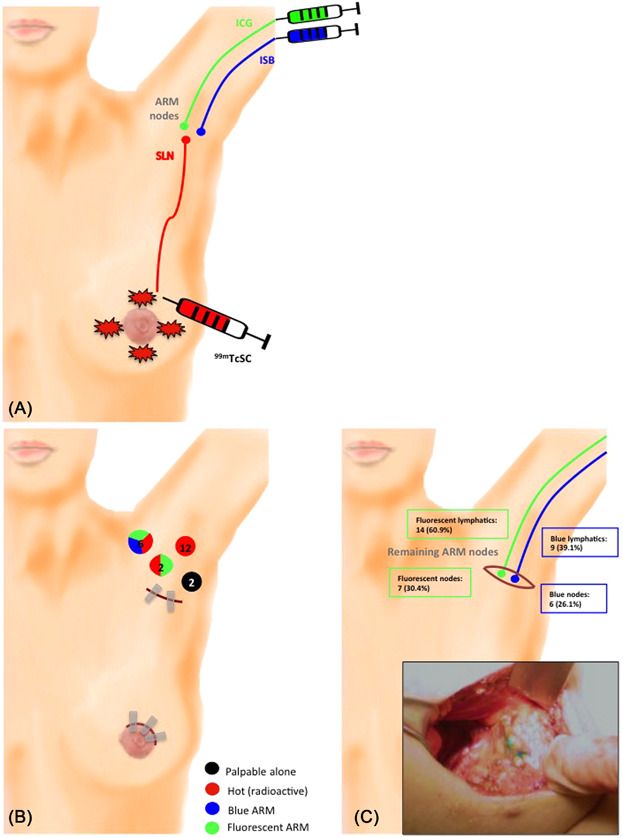
Fig. 1 – Three different markers can be used to differentiate between upper limb and breast lymphatic drainage

Fig. 2 – ARM allows visualisation and sparing of arm drainage during both sentinel node retrieval and axillary lymphadenectomy procedures